In the quiet efficiency of a modern healthcare facility, a single red-capped tube sits on a lab counter, rejected. The diagnosis: Hemolysis.
To the naked eye, it’s just a slightly pink tint to the serum. But in the grand machinery of hospital operations, that one rejected sample is the first domino in a costly, frustrating, and potentially dangerous ripple effect. Hemolysis is responsible for up to 60% of all rejected specimens, leading directly to the operational bottleneck of a redraw.¹
The Physics of “Shear Stress”
If we look beyond the broad statistics, we find that hemolysis isn’t usually a lack of skill, it’s often a matter of physics. We call this “Mechanical Interference.”
Modern collection tubes are designed for high-speed automated labs, utilizing a vacuum to pull blood quickly. However, if the bridge between the vein and the tube isn’t perfectly calibrated, that vacuum becomes a “red cell shredder.” When blood moves too fast through a small-gauge needle or is forced manually through a syringe, the resulting shear stress literally breaks the cells apart. This gap between “volume-based” consumables and “performance-based” results is where the most significant operational waste occurs.
The $4 Million Reality: Quantifying the Leak
While many view a rejected sample as a minor clinical inconvenience, the financial reality is a massive “stealth leak” in the hospital budget. Evidence-based models show that the impact of hemolysis creates a Combined Annual Loss far greater than most administrators realize.
For a typical Emergency Department with 100,000 annual visits and a 7-10% hemolysis rate, the numbers are staggering:
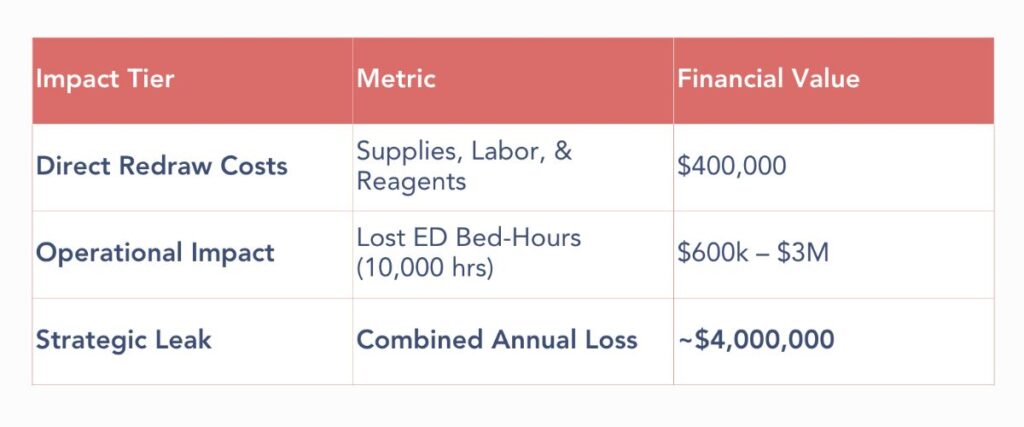
Every hemolyzed sample adds an average of one additional hour to a patient’s stay in the ED. With ED bed-hour costs ranging from $600 to $3,000, the “opportunity cost” of these delays directly affects the facility’s ability to provide timely care and maximize throughput.
Note for Leadership: We have developed a live, interactive version of the logic used in the table above. At the conclusion of this article, you will find access to the 2026 Hemolysis Cost Calculator, where you can input your facility’s specific volume and bed-hour costs to see your custom ROI recovery potential.
Calculation Methodology & Assumptions
To arrive at these figures, our model utilizes evidence-based inputs derived from healthcare finance and laboratory medicine studies.²
1. How We Calculate Direct Redraw Costs
The baseline of $40 per redraw is a conservative industry-standard estimate. This figure accounts for:
- Consumables: New tubes, needles, labels, and tourniquets.
- Clinical Labor: Time required for RNs or phlebotomists to repeat the draw.
- Laboratory Labor: Staff time for processing and the cost of wasted reagents from the initial failed test.
- Context: Redraw-related expenses contribute up to 22.8% of the total cost of serum sample collection.
2. How We Calculate Operational Impact
The primary driver of the $4 million loss is Length of Stay (LOS) impact in the Emergency Department.
- The Time Delay: Research shows patients with hemolyzed samples spend an average of ~1 additional hour in the ED.
- The Opportunity Cost: ED bed occupancy costs range from $600 to $3,000 per bed-hour.
- The Formula: 10,000 hemolyzed samples × 1 hour delay × $600 (conservative bed-hour rate) = $600,000 minimum operational loss.
3. The Model Assumptions (ED Benchmark)
This specific $4 million calculation is based on a published model for a high-volume facility:
- Annual Volume: 100,000 ED visits.
- Testing Rate: 40% of patients receive chemistry panels (40,000 total draws).
- Hemolysis Incidence: A 10% rate (4,000 hemolyzed specimens). Note: Large multicenter studies have recorded rates as high as 17.2%
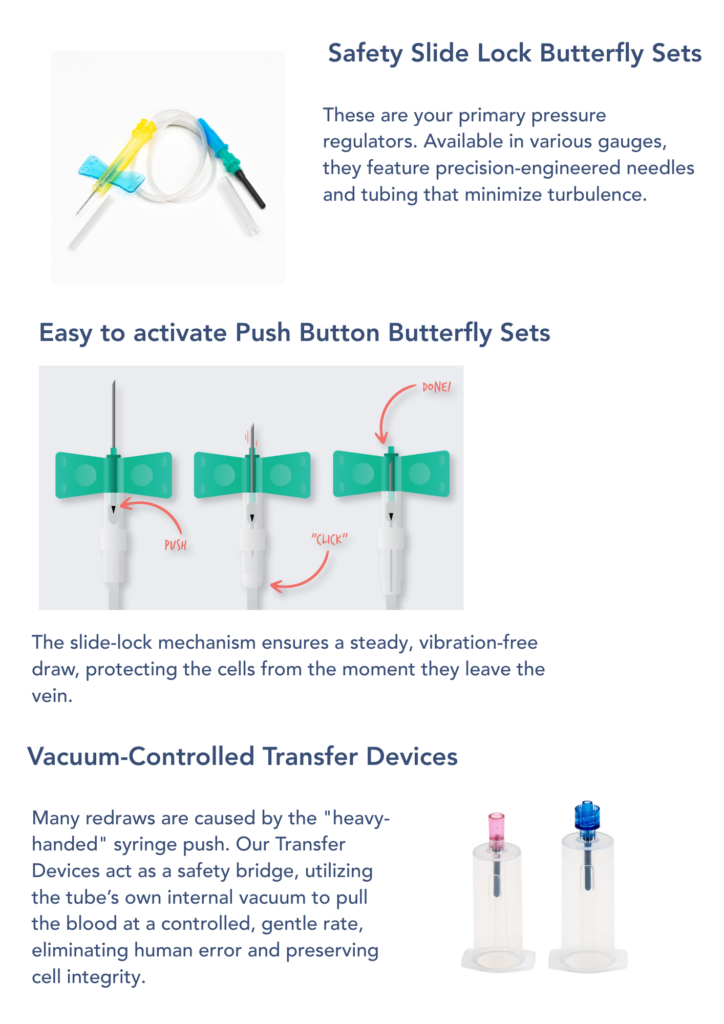
The Caresfield Intervention: Engineering the “Good Draw”
Solving the hemolysis problem requires a specialized toolkit designed to handle the physical stresses of blood collection. At Caresfield, we have engineered a suite of products that act as a protective barrier for every specimen, ensuring that your choice of hardware enhances your facility’s standardization goals.
A Partnership Tailored to Your Story
Every healthcare environment operates with a unique patient volume, a specific staff structure, and existing procurement goals that must be respected. Whether your objective is to optimize system-wide clinical efficiency or you are simply tasked with stopping a multi-million dollar annual budget leak, Caresfield acts as your Unique Alliance. We provide the high-performance hardware and clinical expertise required to bridge the gap between the patient and the lab, ensuring every draw is a successful one.
Audit Your Facility: Access the 2026 Cost Calculator
Don’t leave your operational recovery to guesswork. Use our evidence-based calculator to quantify the “stealth leak” in your department and see the impact of a 20% reduction in hemolysis rates.
Launch the Live Cost Calculator
Put the ROI of Integrity to the Test
Hemolysis isn’t just an “unavoidable cost” of doing business. It’s a preventable process error. We invite you to see how engineered precision can change your lab’s results:
- Consult with Our Experts: Speak to our customer support team about tailored options for your facility. We specialize in finding the best volume-based solutions for your specific budget and clinical goals.
- Request a Sample Kit: Experience the difference that stabilized collection hardware makes in your own environment.
- Launch the Live Cost Calculator: Let us help you calculate the potential revenue recovery of a 20% reduction in your facility’s hemolysis rates.
2 Primary Research Sources
- Journal of Healthcare Finance: This source provides the foundation for the “Direct Redraw Cost” and the “60% Rejection” statistic. It identifies that hemolysis is responsible for up to 60% of rejected specimens. It also establishes that redraw-related expenses (materials and labor) contribute up to 22.8% of the total cost of serum sample collection.
- Academic.oup.com (Clinical Chemistry): This study provides the “Time” and “Throughput” metrics. It confirms that patients with hemolyzed potassium samples spend an average of ~1 additional hour in the ED. It also models the $4 million annual cost impact for an ED with 100,000 visits and a 10% hemolysis rate.
- Europe PMC / Academic.oup.com (Economic Modeling): These sources establish the “Opportunity Cost” of a hospital bed, showing that ED bed occupancy ranges from $600 to $3,000 per bed-hour.
- Journal of Emergency Nursing (jenonline.org): A large multicenter study cited here provides the high-end “Incidence Rate,” recording hemolysis rates as high as 17.2% in some clinical settings.